Deep non-REM sleep is comparable
to the unconsciousness of anaesthesia. In both cases, brain activity slows down
considerably.
Because every stage of sleep has
its own distinctive set of physiological mechanisms, it is hard to establish a
continuum between what might be perceived as lighter and deeper forms of sleep.
According to some criteria, in humans, REM sleep may be regarded as lighter than
non-REM sleep–for instance, it is easier to awaken people from REM sleep
than from stages 3 and 4 of non-REM sleep. On the other hand, the brain maintains
muscle tonus and continues to regulate body temperature during non-REM sleep but
not during REM sleep, so a case could also be made that non-REM sleep is the lighter
of the two.
Because sleep makes animals vulnerable,
the adaptive
advantages that they derive from it must be significant. In terms
of energy conservation, because it is generally colder at night, the lower metabolism
and lower body temperature that characterize sleep might be among the advantages
of sleeping at night.
Moreover, in the course of evolution, homeothermy,
or warm-bloodedness (the ability to maintain a stable body temperature independently
of the ambient temperature) developed at the same time as REM sleep: with the
emergence of birds and mammals. Fish, amphibians, and reptiles, which cannot maintain
a stable body temperature on their own, also do not seem to experience REM sleep.
REM sleep was thus a relatively recent phylogenetic acquisition that complemented
the functions already performed by non-REM sleep.
Hibernation, which
occurs in mammalian species such as hamsters, marmots, hedgehogs, and certain
squirrels, is very different from sleep. When an animal is hibernating, you can
touch it or even move it without its noticing.
Hibernation is a physiological
adaptation that enables these animals to live through winter periods when there
is no food, by reducing their body temperature and hence their metabolism. A hibernating
animal’s body temperature may drop to just a few degrees Celsius, but there
will be a few brief intervals when it rises again. Why? So that the animal can
get some sleep!
Surprising as it seems, while an animal is hibernating,
it accumulates a sleep deficit. When the deficit gets large enough, the animal
emerges from hibernation and sleeps to meet it. These intervals of sleep in the
midst of hibernation represent only about 10% of the animal’s total hibernation
time, but account for a large part of its energy consumption, so they must be
very important indeed for the animal’s functioning.
THE DIFFERENT TYPES OF SLEEP
From a behavioural standpoint,
sleep is defined by four criteria: reduced motor activity, diminished responses
to external stimuli, stereotyped posture (in humans, lying down with eyes closed),
and relatively ready reversibility. These criteria distinguish sleep from coma
and from hibernation (see sidebar).
Compared with wakefulness
and with REM sleep, non-REM sleep is characterized by an electroencephalogram
(EEG) in which the waves have a greater amplitude and a lower frequency. From
the time you fall asleep to the time you reach the deepest non-REM sleep, about
1½ hours later, the amplitude of these waves increases continuously, while
their frequency diminishes correspondingly.
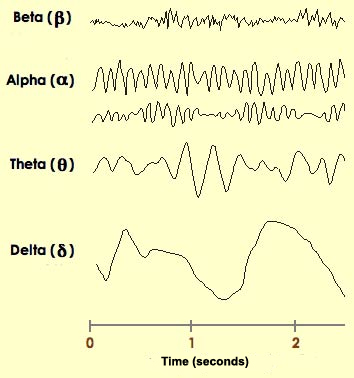
Scientists
have somewhat arbitrarily assigned names to four frequency ranges of waves that
can be distinguished in an EEG trace. From the highest to the lowest frequency,
these waves are as follows.
Beta waves: have a frequency
range from 13-15 to 30 Hertz (symbol: Hz; 1 Hz equals 1 oscillation
per second) and an amplitude of about 30 microvolts (µV).
Beta waves are the ones registered on an EEG when the subject
is awake, alert, and actively processing information. Some scientists
distinguish the range above 30-35 Hz as gamma waves, which may
be related to consciousness–that is, the making of connections
among various parts of the brain in order to form coherent concepts.
Alpha waves:
have a frequency range from 8 to 12 Hz and an amplitude of 30 to 50 µV.
Alpha waves are typically found in people who are awake but have their eyes closed
and are relaxing or meditating.
Theta
waves: have a frequency range from 3-4 to 7- 8 Hz and an amplitude
of 50 to 100 µV. Theta waves are associated with memory, emotions, and activity
in the limbic system.
Delta waves:
range from 0.5 to 3 or 4 Hz in frequency and 100 to 200 µV in amplitude.
Delta waves are observed when individuals are in deep sleep or in a coma.
Lastly, when there are no brain waves present,
the EEG shows a flat-line trace, which is a clinical sign of brain death.
These four types of brain waves, and others discussed
below, are important criteria that have been used to define four distinct
stages of non-REM sleep. Obviously, falling into a deeper
and deeper sleep as the night progresses is actually a gradual, continuous process,
but these four stages still provide a convenient means of describing the relative
depth of non-REM sleep.
Stage
1 non-REM sleep begins when you first lie down and close your eyes. After
a few sudden, sharp muscle contractions in the legs, the muscles relax. Then,
as you continue falling asleep, the rapid beta waves of wakefulness are replaced
by the slower alpha waves of someone who is relaxed with their eyes closed. Soon,
the even slower theta waves begin to emerge.
Though your reactions to
stimuli from the outside world diminish, Stage 1 is still the phase of sleep from
which it is easiest to wake someone up. In experiments where people are awakened
from Stage 1 sleep and asked about their state of consciousness, they usually
report that they had just fallen asleep or had been in the process of doing so.
They also often report having had stray thoughts and short dreams. Each period
of Stage 1 sleep generally lasts 3 to 12 minutes,
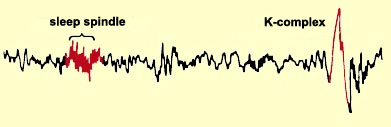
Stage
2 non-REM sleep is a stage of light sleep in which the frequency of the
EEG trace decreases further while its amplitude increases. The theta waves characteristic
of Stage 2 sleep are interrupted by occasional series of high-frequency waves
known as sleep spindles. These bursts of activity have a frequency
of 8 to 14 Hz and an amplitude of 50 to 150 µV. Sleep spindles generally
last 1 to 2 seconds. They are generated by interactions
between thalamic and cortical neurons.
During
Stage 2 sleep, the EEG trace may also show a fast, high-amplitude wave form called
a K-complex. The K-complex seems to be associated with brief
awakenings, often in response to external stimuli.
People in Stage 2 sleep are unlikely to react to a
light or a noise, unless it is extremely bright or loud. It is still possible
to awaken them, even if they then report that they were really sleeping during
the 10 to 20 minutes that this stage lasts during the earliest of the night’s
sleep cycles. But because people go through Stage 2 sleep several times during
the cycles in a night, this is the stage in which adults spend the greatest proportion
of their sleep–nearly 50% of the total time that they sleep each night.
Stage
3 non-REM sleep marks the passage from moderately to truly deep sleep.
Delta waves appear and soon account for nearly half of the waves in the EEG trace.
Sleep spindles and K-complexes still occur, but less often than in Stage 2. The
greater activity observed in the electro-oculogram (EOG) trace during stages 3
and 4 reflects the greater amplitude of EEG activity in the prefrontal areas,
rather than movements of the eyes.
Stage 3 lasts about 10 minutes during the
first sleep cycle of the night but accounts for only about 7% of a total night’s
sleep. During Stage 3, the muscles still have some tonus, and sleepers show very
little response to external stimuli unless they are very strong or have a special
personal meaning (for example, when someone calls your name, or when a baby cries
within earshot of its mother).
Stage
4 non-REM sleep is the deepest, the one in which we sleep the most soundly.
The EEG trace is dominated by delta waves, and overall neuronal activity is at
its lowest. The brain’s temperature is also at its lowest, and breathing,
heart rate, and blood pressure are all reduced under the influence of the parasympathetic
nervous system.
In adults, Stage 4 lasts about 35 to 40 minutes during
the first sleep cycle of the night; it accounts for 15 to 20% of total sleep
time in young adults. The muscles still have their tonus, and some movements of
the arms, legs, and trunk are possible. This is the stage of sleep that accomplishes
most of the body’s repair work and from which it is most difficult to wake
someone up. This is also the stage of sleep in which children may have episodes
of somnambulism (sleepwalking) and night terrors.
Yawning
is a stereotyped behavior with very ancient origins, for it is found
in fish, reptiles, and birds, as well as in humans. Described in ancient times
by Hippocrates (who thought it served to evacuate fever), yawning did not become
a subject of serious interest until the advances achieved in neuroscience in the
1980s.
Generally speaking, yawning consists
of three phases: first, a long intake of air, then a climax, and finally a rapid
exhalation, which may or may not be accompanied by stretching. After yawning,
you generally experience a sense of well being and relaxation and feel much more
present in and aware of your body than you did before you yawned.
Contrary
to what was believed for centuries, yawning does not serve to improve oxygenation
in the brain. This myth was first laid to rest when it was discovered that the
human fetus can yawn as early as the age of 12 weeks, even though it is surrounded
by amniotic fluid in its mother’s belly and so is scarcely likely to get
any more oxygen to its brain from this effort.
Second,
if yawning really helped to raise the oxygen concentration in the blood, then
inhaling pure oxygen would cause yawns to become less frequent, while raising
the concentration of carbon dioxide in the blood would make them more frequent.
But several studies have shown that neither of these things occurs. Also, yawning
is no more common in people with acute or chronic respiratory problems than it
is in the general population.
The role of yawning
has yet to be fully determined. But because we yawn more often when we first awaken,
when we are bored, and when we are trying not to fall asleep, its primary function
would appear to be to help make us more alert. Yawning also seems to play a role
in non-verbal communication, especially among primates.
Which
leads us to something truly singular about yawning: its contagiousness. That is,
when we see someone yawn, it makes us yawn. Sometimes simply thinking about a
yawn can be enough to trigger one! Obviously, the term “contagiousness”
should not be taken literally here, because no germs are being transmitted. More
precisely, yawning is a form of involuntary imitation.
Some scientists believe that this characteristic of yawning may have developed
as a mechanism for promoting social cohesion, for example, by enabling all the
people present in a group to have the same level of alertness at the same time.
In the rest of the animal kingdom, yawning is observed
among predator and prey species alike. Among predators, its purpose might be to
encourage the group to take a restorative nap so that all of its members can be
well rested for an attack on their prey later on. Among prey, by encouraging all
members of the group to fall asleep at the same time, yawning might reduce the
risk that any one individual might be sleeping alone and hence highly vulnerable
to attack by a predator.
There is no nerve centre
strictly associated with the yawn reflex, but certain brain structures, such as
the hypothalamus, the pituitary gland, and the brainstem are essential for its
expression. Some scientists have even hypothesized that the strong contractions
of the jaw muscles during yawning may stimulate the reticular formation and thereby
encourage wakefulness.
Lastly, one interesting linguistic
note: the French verb bâiller (to yawn) has a circumflex accent
on the “a” and not on the “i” because in Old French, when
people pronounced this word, they stretched out the “a” to imitate
the sound of someone yawning.
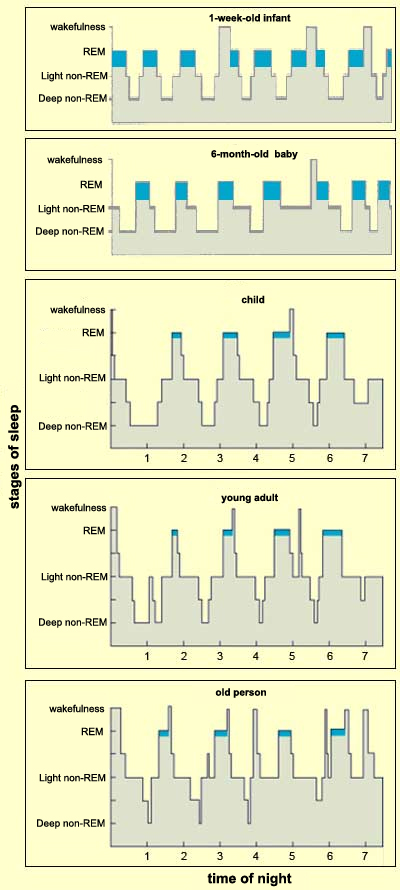
In young adults, REM sleep accounts
for 20 to 25% of total sleep time, but in newborn infants, it accounts for 50%.
Newborns sleep about 16 hours per day and hence spend about 8 hours per day in
REM sleep! The proportion of REM sleep is apparently even higher before birth,
because babies who are born prematurely spend up to 80% of their sleep time in
REM sleep. We have no way of knowing, however, whether
this REM sleep is accompanied by dreams.
In reality,
the percentage of REM sleep stabilizes at around 20 to 25% at about age 10. After
age 60, this percentage declines significantly, until at age 70, people get only
about 45 minutes of REM sleep per night.
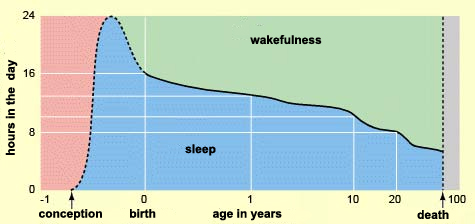
THE SLEEP CYCLES IN A NIGHT
How much time people
sleep at night varies greatly with their age. Broadly speaking, from birth to
death, the amount of sleep we get each night decreases steadily.
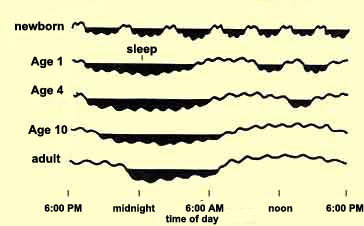
Newborns
sleep an average of 16 hours per day, but even at this age, some babies sleep
a lot more (20 hours) while others sleep a lot less (12). Newborns’ sleep
is not affected by the alternation of day and night. Instead, it is broken up
into periods of 3 or 4 hours, and the main thing that wakes newborns up is the
need to nurse. Infants spend about half of their sleeping lives in REM sleep–double
the proportion for adults.
Babies
develop a circadian rhythm when they are somewhere between 1 month and 6 months
old. At that point, they begin to sleep through the night (much to their parents’
relief) and their sleep becomes mainly nocturnal (for example, 10 hours through
the night, and 2 or 3 naps for a total of 6 hours in the daytime).
The
average amount of sleep that children get per day declines steadily as they grow
older–from 15 hours when they are 6 months old, to 14 when they are 2 years
old, and then to 12 (10 hours at night and a 2-hour nap in the daytime) when they
are about 3 or 4 years old. Their proportion of REM sleep declines rapidly until
age 4, when it stabilizes at the same level as a young adult’s: about 20
to 25% of the total time spent asleep.
Children around 10 years old
sleep just about 10 hours per night. Teenagers still need more sleep than
adults–around 8½ to 9 hours. Teens’ biological clocks also
make them stay awake later into the night and stay asleep later into the morning.
That’s why classes that start early in the morning aren’t the greatest
idea for teenage students.
In older people, sleep is
often lighter and more fragmented. Older people also tend to get up earlier in
the morning. They don’t sleep as long at night, but they continue to need
about the same total amount of sleep as young adults, and therefore need to take
naps in the daytime to make up for their shorter sleep at night.
Source:
adapted from Challamel M.J., Thirion M. and Appleton & Lange, Kandel, Schwartz,
Jessell, Principles of Neural Science
In
older people, REM sleep decreases to about 15% of total sleeping time. The
deepest form of sleep (Stage 4 non-REM sleep)
also diminishes gradually with age, so that older people’s sleep is more
susceptible to disturbances of all kinds. Given the importance of non-REM sleep
for the immune system, it may well be that this reduction in non-REM sleep also
makes older people more vulnerable to illness.
The dream theories of Mark Solms
and Jean-Pol Tassin (described to the right on this page) are consistent not only
with certain aspects of psychoanalysis, but also with models in which nocturnal
brain activity reactivates what we have learned during the day, thus consolidating
certain memories and actions. Because dreams do not seem to reactivate these memories
randomly. Instead,
the memories that have been associated with the most intense emotions, whether
very early in life or during the days immediately preceding the dream, appear
to be activated preferentially.
Other experiments,
using brain imaging, have shown that during REM sleep, the limbic
system, which is heavily involved in emotion and motivation, is very active,
while some areas of the prefrontal cortex that are involved in working
memory, attention, logical reasoning, and self-control are, in contrast, inactive.
This suppression of activity in the prefrontal cortex might explain several characteristics
of dreams, such as their strange imagery and absence of logic and self-criticism,
not to mention how quickly they fade when you wake up.
These
findings are thus consistent with a number of elements of classical Freudian dream
theory, such as the ideas that our desires and motivations are encoded in our
dream images and that we are emotionally disinhibited when we dream.
The
reduced activity in the frontal lobes that is observed in brain images captured
during REM sleep does not seem to support Solms’s observations that ascribe
a role to this area in the generation of dreams. Further studies will therefore
likely be needed to define the role that the various regions of the frontal lobes
play in dreams.
DREAMS
What purpose do dreams serve?
And does it even make sense to begin with to ask whether dreams serve a biological
function just like eating and breathing, for example?
Some
neurobiologists say not, seeing dreams as mere epiphenomena associated with brain
activity. But others think that dreams contribute
to epigenetic development or to the processing of recently acquired information.
Still others have taken neurobiological data from brain-imaging studies done in
the 1990s and used these data to support a theory holding, as Freud did, that
dreams are psychological manifestations that can convey meaning.
One
such theorist is neuropsychologist and psychoanalyst Mark Solms.
Solms first observed that a number of his patients who had suffered damage to
the neurons of the pons and therefore no longer had any periods of REM sleep nevertheless
continued to dream regularly. He then identified two areas of the cortex that
had nothing to do with REM sleep but that, when damaged, caused the loss of the
subjective experience of dreaming.
The first of these
areas is located where the occipital,
temporal, and parietal cortexes meet. This area is involved in spatial imagery,
among other things, so Solms’s finding makes intuitive sense: it is hard
to imagine being able to dream if your ability to form mental images were impaired.
The other area of the brain that seems to be necessary
for dreaming, according to Solms’s research, is located in the frontal
cortex. The neural pathways that project to this area use dopamine
as a neurotransmitter and are known as the mesolimbic
system. The area itself is involved in positive
reinforcement and motivation.
Why
then should dreams disappear when this part of the brain is damaged? Probably
because dopaminergic transmission has been disrupted. In any case, that is what
is seen in people who take medications known to decrease their dopamine levels:
they dream far less. And the opposite is also true: patients who take medications
that increase dopaminergic activity along this pathway (for example, Parkinson’s
patients who take L-dopa) dream more intensely than they used to, even though
the frequency and duration of their periods of REM
sleep are unchanged.
For Solms, it therefore seems
clear that if REM sleep is generated in the most ancestral parts of the brainstem,
dreams, in contrast, may arise in the cortex. The involvement
of the frontal and the occipito-temporo-parietal cortexes, which regulate memory,
feelings, and motivation, supports the idea that dreams in some way serve to reprocess
subjective events that the individual has experienced previously. In short, Solms’s
theory allows for the possibility that dreams may have meaning and thus preserves
the foundations of psychoanalysis, in contrast to Hobson
and McCarley’s model, in which dreams are simply the result of the random
bombardment of the cortex by meaningless signals from the pons.
This
theory of the cortical origin of dreams raises several issues. One in particular
is the difficulty of reconciling the very fleeting nature of our memories of our
dreams with the very fundamental role that this theory implies dreams play in
our psychic equilibrium.
The strange and fragmentary
nature of our dreams as we recollect them is central to another daring theory
of their origin: we may dream not when we are sleeping, but only as we
are awakening. This theory, developed by French neuroscientist
Jean-Pol Tassin, is based on the paradox that consciousness vanishes
during sleep, yet dreams cannot exist unless we are conscious of them. According
to Tassin and his collaborators, during REM sleep, the brain is active, but its
activity allows neither consciousness nor dreams.
There
is a neurobiological correlate that supports this interpretation: some
noradrenergic and serotonergic neuromodulatory neurons that are necessary
for neural information to be stored in the brain for more than a few milliseconds–in
other words, necessary for consciousness–cease to function when you are
asleep, but become active again while you are waking up.
Thus,
according to Tassin’s theory, as you awaken, these reactivated neurons enable
you to become aware of the subliminal images generated during your sleep, and
you then actually construct your dreams during the few hundredths of a second
that it takes you to wake up. This brief interval might also be the time when,
as sometimes happens, you incorporate into your dreams the light or the words
that have woken you up.
But how then to explain the
subjective impression that we dream during the night? Researchers who have analyzed
EEG traces for entire nights of sleep have found that even sound sleepers may
awaken as many as 10 times per night, then fall back to sleep again rapidly, even
if the next morning they report that they slept straight through the night. During
these “micro-awakenings” that last only a few seconds or fractions
of a second, the brain finds itself in a state identical to wakefulness, but for
such a short time that we very rarely remember it the next day. It would be during
these micro-awakenings that we might dream, that is, organize our often bizarre
mental images into coherent stories. And as the generator of these bizarre mental
images, REM sleep seems the ideal candidate, though
non-REM sleep can generate some strange images too. What makes this theory
even more plausible is that REM sleep is the phase of sleep in which spontaneous
awakenings are the most frequent.
This model thus provides
an explanation for the illogical, impossible or unreal nature of the story lines
of most of our dreams: because the return to consciousness that gives rise to
dreams occurs in a very short time span, often following a period of REM sleep,
the images we remember are too disparate to be integrated into a coherent story,
and our conscious brain may therefore have to “force” reality a bit
to assign a meaning to them. This would not be the only instance in which the
brain plays tricks on us in an attempt to give a meaning to confusing stimuli;
certain
optical illusions and split-brain experiments offer other examples of this
same phenomenon (follow the Experiment Module link to the left).
For
Tassin, dreams would thus represent the conscious expression, during awakening,
of the unconscious brain activity that occurs while we are asleep. Dreams would
thus remain dependent on sleep, because they would arise from the sudden reactivation,
at the moment of awakening, of the serotonergic and noradrenergic neurons whose
activity is indispensable for consciousness.
If this
theory proves correct, many observations could be interpreted differently. For
example, when you awaken someone who is sleeping, you aren’t interrupting
her dreams, but rather making them happen! And Jouvet’s
sleeping but “disinhibited”cats were simply reproducing movements
that they also made during the daytime, without consciously perceiving images
associated with these movements–in other words, without dreaming.
This
view of dreams has the further advantage of leaving open the possibility that
dreams may have a meaning for the people who dream them. Because if their dreams
occur in the space of a few hundred milliseconds, then the mental censor that
may be active when they are awake is not in place, thus allowing bizarre dream
content that might be worth interpreting.
Narcolepsy occurs
just as commonly as Parkinson’s disease and multiple sclerosis, but much
less is known about it. It is often confused with other pathologies such as epilepsy
and often takes more than 10 years to be diagnosed accurately. This disease does
seem to have a genetic component, but its expression is likely influenced by environmental
factors as well.
Here is an example of a
case of narcolepsy reported by a physician. The patient, a French shepherd
about 30 years of age, said that he would sometimes discover that he had been
sleeping standing up while he was supposed to be watching his herd. He also sometimes
had strange visions, dreamt while he was walking, or suddenly found himself standing
in the kitchen of a neighbouring farmhouse, without knowing how he had gotten
there. Once, he had fallen on the floor in the middle of a conversation with the
clerk at the post office. When he felt like laughing, or was angry, his legs would
often tremble, and he would collapse like a marionette whose strings had been
cut. At night, he slept poorly and sometimes felt as if he were paralyzed.
Narcolepsy is also seen
in animals, including goats, donkeys, ponies, and several breeds of dogs
that display a genetic disorder with symptoms similar to those of narcolepsy in
humans. These breeds of dog were discovered to have a mutation on the hypocretin
receptor 2 gene.
Hypocretin is a neurotransmitter
that is synthesized solely by the neurons of the hypothalamus that project to
structures involved in various aspects of sleep. Normally, the secretion of hypocretins
helps to maintain muscle tonus and alertness by activating monoaminergic and cholinergic
neurons. Apparently, the mutation of the hypocretin receptor 2 gene causes hyperexcitability
in the neurons that generate REM sleep and alters the circuits
that inhibit REM sleep. In humans, the degeneration of the neurons that produce
hypocretins would have the same effect.
SLEEP DISORDERS
Since the 1970s, laboratories
that do research about sleep have been established in many parts of the world.
Thanks to their discoveries, we now know that the
health problems caused by lack of sleep are far more numerous than we once
imagined. These laboratories have also identified over 100 different disorders
that can affect our sleep. Besides insomnias
and disturbances in circadian rhythms, hypersomnias and parasomnias
represent the two other main categories of sleep pathologies.
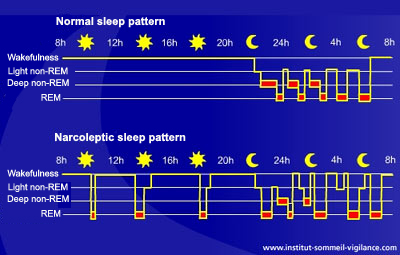
Narcolepsy, formerly called “sleeping sickness”, is a hypersomnia
that is characterized by excessive sleepiness during the day and, in extreme cases,
by sudden irresistible bouts of sleep that occur several times per day. People
with narcolepsy can thus literally fall asleep at any time. In addition, during
these attacks, they pass directly from a state of wakefulness to a state of REM
sleep, unlike healthy people, who always go through
a period of non-REM sleep first. In fact, many of the symptoms of narcolepsy
can be seen as the intrusion of a phase of REM sleep into a person’s waking
life.
More
and more studies in animals and humans (see sidebar) tend to suggest that hypocretins
(also known as orexins), a class of neuropeptides produced solely by
the neurons of the hypothalamus, play a role in narcolepsy. Several post mortem
analyses have found far fewer of these neurons in the brains of people with narcolepsy
than in those of healthy persons.
In its most complete
form, narcolepsy is also accompanied by a condition that is startling, to say
the least, to those who witness it: cataplexy, a sudden decrease
in muscle tonus, varying in intensity and lasting less than a minute. The signs
of cataplexy range from a simple weakness in the neck, knees, or facial muscles
to total paralysis that causes the individual to fall to the ground.
An attack of cataplexy is usually caused by a strong emotional trigger such as
laughter, anger, surprise, or sexual arousal. People having a cataplectic attack
are often still conscious but unable to move, which makes this condition fairly
terrifying. Once again, the connection with REM sleep is quite apparent: muscle
atonia in all respects similar to that which occurs during REM sleep to prevent
our bodies from acting out our dreams.
Sleep
paralysis and sleep hallucinations are other symptoms
of narcolepsy. Sleep paralysis is a temporary inability to speak or to move while
falling asleep or waking up–a highly disconcerting experience, especially
when the person having it doesn’t know its cause. Sleep hallucinations are
strange, unpleasant experiences that resemble waking dreams. They occur during
the transition from waking to sleeping, as well as during periods of reduced alertness
in the course of the day.
Parasomnias is an umbrella term
for a variety of abnormal phenomena that occur during sleep. Several types of
parasomnias affect children in particular. One example is night terrors, a phenomenon
completely different from simple nightmares.
The Nightmare, by Heinrich Füssli (1792). Private collection.
Nightmares
are dreams involving visual images that are frightening enough or negative emotions
that are strong enough to cause the dreamer to wake up scared and anxious. This
feature differentiates a nightmare from a simple bad dream that doesn’t
cause the dreamer to wake up. In children, nightmares are associated with normal
aspects of psychological development, such as separation anxiety or sibling
rivalry. In adults, nightmares tend to be precipitated by stress or by physical
factors such as fever. Some violent, recurring nightmares may also be related
to post-traumatic
stress.
Night terrors
are events that are biologically and psychologically distinct from nightmares.
They begin when children are 3 to 6 years old and generally disappear during adolescence.
Children in the throes of a night terror scream and cry. Their eyes are open,
and they may say incoherent things while gesturing emphatically. Unlike nightmares,
of which people can clearly recall some details once they awake, night terrors
are characterized by confusion upon awakening, the lack of any recall of elaborate
dream imagery, and intense activation of the autonomic nervous system, causing
symptoms such as sweating, and elevated heart rate and blood pressure. Also, nightmares
occur mainly during periods of REM sleep in the second half of the night, whereas
night terrors typically occur during deep (Stage 3 and Stage 4) non-REM sleep,
during the first part of the night. An entire night-terror episode can last 1
to 20 minutes. The next morning, the child usually wakes up in a good mood, having
forgotten the entire incident.
Enuresis (involuntary bed wetting
during the night) of course does leave obvious traces the next morning. Children
are diagnosed as enuretic if they wet the bed more than twice per week after age
5 or 6–in other words, long after they are toilet-trained. The best approach
to this problem is not to punish or humiliate the child, but rather to be supportive
to help maintain the child’s self-esteem. This problem generally disappears
on its own by adolescence.
Somnambulism
is another form of parasomnia that is especially common in children. It involves
sleepwalking during non-REM sleep. About one-third of all children display this
behaviour at some time or other, and about 3% do so at least once per month. As
with enuresis, episodes of somnambulism generally disappear gradually as the child
grows older, so that only 1 to 4% of adults still have them occasionally.
Contrary
to popular belief, it is not dangerous to wake up someone who is sleepwalking.
But it can be fairly hard to do so, because episodes of somnambulism, which generally
last about 10 minutes, typically occur during the deepest stage of non-REM sleep,
Stage 4, and hence during
the first sleep cycles of the night. Thus somnambulism is neither caused nor
accompanied by dreams.
Episodes of somnambulism are
believed to be triggered when something such as a noise, or the need to urinate,
wakes up the body without waking up the brain. The sleepwalker may then get up,
walk to the kitchen, open the fridge, eat a snack, pick up the telephone, or play
some music, with no conscious awareness of any of these actions. Because this
state of very partial cognitive functioning obviously entails some dangers, the
best thing to do with a sleepwalker is gently guide him or her back into bed.
Somniloquy–talking
in one’s sleep–can happen during either REM or non-REM sleep. The
words are generally so poorly articulated and the sentences so meaningless that
anyone who hears them will be at a loss to interpret them. Those utterances that
occur during REM sleep do, however, tend to be somewhat more intelligible.
Bruxism is a strange parasomnia.
It consists in repetitive, involuntary grinding of the teeth that causes them
to suffer abnormal wear and tear and also causes discomfort in the jaw muscles.
Though about half of all people move their jaws in their sleep, only about 6%
display the tooth-grinding during the light stages of non-REM sleep that characterizes
bruxism. The mechanisms of this disorder are not yet fully understood, though
it is now agreed that they do originate in the central nervous system. People
who suffer from bruxism will generally benefit from reducing their stress and
from wearing a special device in their mouth to prevent tooth damage.
REM sleep behaviour disorder is
a rare but fascinating pathology sometimes seen in older people. It consists in
a form of sleepwalking that may superficially resemble somnambulism, but is significantly
different, because the people engaged in this behaviour are in REM sleep rather
than non-REM sleep. Normally, during REM sleep, people’s muscles are completely
paralyzed, except for those involved in respiration and in moving their eyes.
But individuals who suffer from REM sleep behaviour disorder do not experience
this characteristic paralysis. Instead, they literally jump out of bed and mime
their dreams while continuing to sleep! This disorder is very dangerous, because
people who have it often injure themselves while externalizing their dreams, attempting
to fight or flee some non-existent assailant. Sometimes the dreamers may cast
their bedmates in the role of the assailant, who may then find his or her own
dreams rudely interrupted! Luckily, this condition does respond to some medications,
such as the benzodiazepine
clonazepam.
Sleep
paralysis, which is very common in people with narcolepsy, can also occur
in isolation, with no other associated pathology. This parasomnia is manifested
when the individual is falling asleep or waking up, and it typically lasts just
a few minutes. During this period, the person can neither move nor speak. This
paralysis of course causes significant anxiety. It may also be accompanied by
visual, auditory, and even tactile hallucinations, known as hypnagogic hallucinations.