Non-REM sleep accounts for about
75 to 80% of your total sleep each night, or about six hours of non-REM sleep
if you sleep eight hours in total. You spend the remaining two hours–roughly
20% of the night–in REM sleep.
It seems that with training, people
can gradually reduce their normal amount of sleep by an hour or two without feeling
too tired.
The main difference between being
awake and being asleep is that in the latter state, consciousness does not intervene.
When you’re asleep, it’s somewhat as if your brain were closing itself
off and becoming a sort of “temporary autonomous zone”. But in reality,
your brain is never completely cut off from the rest of the world: even during
the deepest stages of sleep, a strong enough stimulus from your environment will
be perceived by your brain and may cause you to wake up.
On every normal day
of our lives, each of us engages in two very distinct kinds of behaviours:
sleeping and being awake. On the surface, these two behaviours are so different
from each other that even extraterrestrials who came to observe life on Earth
would notice the difference right away. The entry in their ship’s log might
read: “Earthlings spend about two-thirds of each day upright and moving
around and the other third lying down and still.”
But
what these extraterrestrials would not notice right away, and what even Earth’s
own scientists did not begin to discover until the mid-20th century, is that sleep
is far from a simple matter of placing our mental and physical activities on hold.
Sleep is a genuine “second state", just as varied and complex as the
state of wakefulness, and characterized by major changes in physiological characteristics
such as body temperature, hormone secretions, heart rate, and respiration rate.
Also, far from being uniform, sleep rotates through various stages that
occur in a characteristic order in the course of the night.
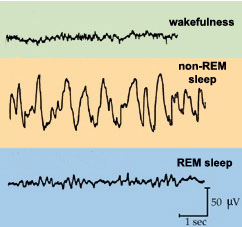
The
stages of sleep that occur after you first fall asleep consist of what is called
non-REM sleep, or slow-wave sleep. The slow waves in question
are the ones seen on the electroencephalogram (EEG) trace (follow the Tool Module
link to the left) of someone who is in these stages of sleep; this trace consists
of very slow, high-amplitude oscillations.
These stages
of non-REM sleep are followed by a stage of another kind of sleep, in which, paradoxically,
the EEG trace looks much more like that observed in people who are awake: the
waves are faster, and their amplitude is smaller. Hence this kind of sleep is
often known as paradoxical sleep, the name that it was given
in 1959 by Michel Jouvet, a French neurobiologist who conducted the first animal
experiments concerning it. But this form of sleep is also characterized by numerous
rapid eye movements (REMs) that take place underneath the closed eyelids, and
hence is usually referred to as REM sleep. Probably the most
fascinating characteristic of REM sleep is that it is the stage of sleep in which
we experience our most detailed and strangest dreams.
Thus scientists go beyond the observations
of our hypothetical extraterrestrials and distinguish not just two but three fundamental
behavioural states: wakefulness, non-REM sleep, and REM sleep. Each of these states
is generated by a specific pattern of brain activity and accompanied by specific
changes in the activity of the body as a whole.
The
average adult human sleeps 7 to 8 hours per night. But about 10% of the adult
population needs much more sleep at night –9 or even 10 hours–to feel
wide awake during the day. At the other end of the spectrum, some 5% of the population
can get along fine with only 5 or 6 hours of sleep. Thus there is no particular
amount of sleep that is ideal in itself. The only real criterion for whether you’re
getting enough sleep is whether you feel in good shape during the day.
The
variations in the amount of sleep that people need are determined both by their
genetic make-up and by their lifestyle, especially during adolescence. The same
goes for people’s tendency to go to bed early and wake up early, or to go
to bed late and wake up late. Thus it would be just as silly to say that everyone
should sleep 8 hours, from midnight to 8:00 AM, as it would be to say that everyone
should wear the same style of shoe, in a size 8.
But regardless of whether
people sleep 6 hours or 10 hours per night, they all get about the same amount
of deep non-REM sleep: 100 minutes. People who sleep more total hours each night
devote some of the extra time to REM sleep, but more of it to light non-REM sleep.
Thus people who sleep less might be said to have a higher concentration of deep
non-REM sleep than people who sleep more.
In today’s performance-obsessed
society, people often cite Napoleon, Louis XIV, and Churchill as examples of high
achievers who supposedly slept only a few hours each night. But curiously, people
fail to mention all the other high achievers who, like Einstein, needed 10 and
sometimes even 12 hours of sleep per night!
For most people, the length of their
sleep cycles remains relatively constant, night after night, throughout their
lives. Some people have 90-minute cycles, while others have cycles of 100, or
110, or 120 minutes, and so on.
People
who need lots of sleep and people who need less sleep all get just
about the same number of hours of deep non-REM sleep each night. Thus it is REM
sleep and especially Stage 1 and Stage 2 non-REM sleep that vary the most from
one person to another and that are curtailed in people who sleep fewer hours per
night.
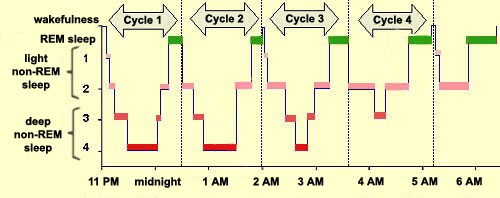
To better visualize these general patterns, researchers
use a type of graph called a hypnogram. A hypnogram is nothing
more than a minute-by-minute graphic record of a night’s sleep, as captured
by an EEG. The hypnogram thus shows not only the sequence in which the various
stages of sleep occur, but also the times at which each stage starts and ends.
Another striking feature of the hypnogram is the recurrent cycles
in which the various stages of sleep follow one another, somewhat like a series
of waves: 1-2-3-4-3-2-1-REM-1-2-3-4-3-2-1-REM, etc. Thus each descent into deep
non-REM sleep is followed by a climb back up directly into a period of REM
(or paradoxical) sleep.
The “train” of a night of sleep comprises
many “cars” that are linked to one another in a specific order to
form 4 or 5 major cycles.
Each cycle lasts
about 1.5 to 2 hours, and a person thus goes through 4 or 5 of these cycles in
one night’s sleep. Such cycles are described as “ultradian rhythms”,
in contrast to the longer circadian rhythms, which have a period of about 24 hours.
The
hypnogram also shows that deep non-REM sleep (Stages 3 and 4) is deepest
in the earlier part of the night. This explains the great physically restorative
powers associated with the first few hours of sleep. Toward the end of the night,
the pattern reverses, and REM sleep, the kind of sleep generally associated with
dreaming, becomes predominant.
We all dream every night, even if
we don’t remember our dreams. Memories of dreams are very unstable
and disappear within a few minutes after we wake up. But it’s relatively
easy to remember your morning dreams, either by writing them down as soon as you
wake up, or by repeating
their content to yourself so that they leave a trace in your long-term
memory.
The worries that we experience during
the day are often incorporated into our dreams. U.S. psychologist Rosalind Cartwright
studied a large number of individuals who were going through divorces, and she
found that when these people were awakened from REM sleep, most of the dreams
that they reported dealt with their marital concerns.
In experiments that he conducted
in the 1960s using cats, French neurobiologist Michel Jouvet succeeded in destroying
the
part of the brain that is responsible for the generalized absence of muscle tonus
during REM sleep.
This operation did not affect REM sleep in any other way; it continued normally,
except that the cats’ muscles could now contract. What happened then? With
the inhibition on their muscle movements removed, when the cats entered REM sleep,
they would raise their heads, get up, and arch their backs, clean themselves,
or stalk imaginary prey! In short, they engaged in the usual behaviours that characterize
their species when awake.
At the time, Jouvet had concluded that the cats
were “living their dreams”, and he thus associated REM sleep with
dreaming. But more recent findings have
raised questions about this interpretation.
DREAMS
Since
ancient times, dreams have often been regarded as divine messages. With the
work of Freud in the
early 20th century, dreams came to be seen as the “royal road to the
unconscious”. In the Freudian view, we construct the plots for our dreams
both from impressions that we have gathered in the course of the day and from
older memories that have been transformed or disguised to escape the control of
our conscious minds.
It was not until some 50 years
later, with the discovery of REM
(paradoxical) sleep in 1953, that dreams were first associated with an observable
physical state of the brain.
Henri Rousseau (1844-1910), The
Dream, 1910; Oil on canvas, 6’8½” x 9’9½";
The Museum of Modern Art, New York.
The
decisive experiment that established this connection was conducted by Nathaniel
Kleitman and Eugene Aserinsky, the two U.S. physiologists who had discovered REM
sleep. Their experimental protocol was quite simple: when the human subjects who
were sleeping in their laboratory displayed the rapid
eye movements typical of REM (paradoxical) sleep, the researchers woke them
up and asked them whether they had just been dreaming. Some 75 to 95% of the subjects
answered that they had indeed been dreaming, and were able to recount vivid dreams
whose content was often fantastic, filled with all kinds of details and emotions.
This discovery received huge attention,
because it was the first time that anyone had made an association between quantifiable
states of REM sleep and what people experience subjectively as dreams.
But
the mystery of dreams was still far from solved, because there were still some
5 to 10% of subjects who, though awakened from stages of non-REM
sleep rather than REM sleep, nevertheless said that they had been dreaming.
This percentage was even higher–as high as 70%–when instead of asking
the subjects “Have you been dreaming?”, the researchers simply asked
them “What was passing through your mind?” The states that the
subjects reported in these cases were like sensory impressions similar to the
dreams of REM sleep, but of shorter duration and with a more concrete, logical
structure.
Thus REM sleep is not necessary
for dreaming. A certain kind of dream (one involving surprising juxtapositions)
does seem to be closely associated with REM sleep, but dreaming and REM sleep
are in no way synonymous. This distinction between dreaming,
which is a subjective state, and REM sleep, which is
a state of the brain, is fundamental. In other words, dreaming is a phenomenon
that can be described only qualitatively, by the dreamer himself or herself, in
an account that often involves some distortions, whereas REM sleep can be subjected
to precise physiological measurements, in particular by means of its
EEG trace.
It turns out that counting sheep
isn’t really that much of a help in falling asleep–it’s more
of a distraction.
Source: www.ahajokes.com
There are plenty of stories about
people who went several days without any sleep. In 1959, a disc jockey in New
York stayed awake for a week as a fundraising stunt for a charity. The researchers
who monitored him closely during this experiment found that he soon began to have
hallucinations, and then became so paranoid that he refused to answer their questions.
Dr William C. Dement, an important sleep researcher, used himself as
the subject of a sleeplessness experiment. After 48 hours without sleep, he confirmed
that he was experiencing feelings of paranoia and suspiciousness toward his roommates.
Very soon, he also experienced problems with his vision, as well as being unusually
distracted and clumsy.
But the longest documented voluntary period of
sleeplessness involved a 17-year-old male from California who went 264 hours (11
days!) without sleeping. He did so on a bet, and he did not use any stimulants
to accomplish this feat. When he was done, he slept like a rock for 15 hours,
and after a few more nights of sound sleep, he was as good as new.
Driving when you haven’t had
enough sleep is definitely a bad idea. In the United States, an estimated 56 000
highway accidents per year, involving some 1 500 fatalities, are believed
to be caused by drivers who have fallen asleep at the wheel.
If you’re
feeling sleepy while you’re driving, turning on the radio and opening your
window will rarely suffice to keep sleep at bay. The best thing to do is stop
your car on the side of the road and take a 15 to 20-minute nap. Drinking a cup
of coffee
may also help for a few hours, but coffee needs about 30 minutes to take effect.
Thus one good way to refresh yourself a bit for the road is to drink a cup of
coffee, then take that nap while you wait for the coffee to kick in.
Sleep restriction therapy
is a behavioural approach to treating insomnia. For example, suppose
you’re sleeping only 6 hours per night because it’s taking you 2 hours
to fall asleep. In this form of therapy, you would let yourself stay in bed for
a total of only 6¼ hours. So if you always got up at 7:00 AM, you wouldn’t
let yourself go to sleep until 12:45 AM. This restriction would help you to short-circuit
the idea of performance associated with sleep, while aggravating your sleep deprivation
very slightly. After a few nights of such treatment, people who have been experiencing
insomnia often fall asleep in less than 15 minutes. They then gradually lengthen
the amount of time that they stay in bed, by 15 minutes each week, until eventually
they are getting a reasonable night’s sleep.
SLEEP DISORDERS
People are too quick
to label others as lazy if they accord a lot of importance to their sleep. When
we’re short of time, our hours of sleep are often one of the first things
we let go. But if there’s one thing for which we should show more respect,
it’s our need for a good night’s sleep.
To understand the importance of sleep, simply
consider what happens to people who don’t sleep enough (or, as the medical
profession might put it, people who show signs of sleep deprivation syndrome).
Obviously, these people feel sleepy during the daytime. They may also tend to
“sleep in” on the weekend to pay back their “sleep debt”.
If they don’t manage to pay back this debt,
they will suffer several harmful consequences. First, they’ll be less alert,
and their ability to think and concentrate will be diminished. Next, their reflexes
will slow, and they will experience memory
disorders, muscle fatigue, and mood swings, and even display aggressive behaviour
and have difficulty in situating themselves in time or space. They may also experience
hallucinations similar to those that most people experience when falling asleep,
midway between reality and dreaming. Such hallucinations are harmless when you’re
in bed, but can be fatal if you’re at work or at the wheel (see sidebar).
In fact, it is believed that lack of sleep may be the hidden cause behind most
of the “human
error” that causes accidents.
In the longer
term, several studies have found, there is a relationship between insufficient
quantity and quality of sleep and a number of chronic health problems, including
obesity, diabetes, and high blood pressure. In these three cases, the lack of
sleep disturbs regulatory mechanisms that are normally at work during the night.
Lack of sleep may be voluntary or involuntary. You
may cut back on your hours of sleep voluntarily when you work
too far into the night, or when you stay up late to pursue more entertaining nocturnal
activities. But lack of sleep can also be involuntary, when
you try to sleep but can’t manage to do so–in other words, when you
experience insomnia.
Insomnia often sets in insidiously. Suppose, for example,
that at first you lose a few nights because you’re worrying about having
lost your job, or about your daughter’s marital problems. After a few nights,
when you go to bed, you might also start worrying about whether you’ll be
able to fall asleep. These worries might be bad enough that they will in fact
make it harder for you to sleep. Having had yet another bad night’s sleep,
you’d go to bed even more worried the next night, and the vicious cycle
of insomnia would be well under way.
More than half
of all people with insomnia can obtain some relief, if not a complete cure, by
simply applying the following recommendations for healthy living, which involve
changes both in attitudes and in habits. This “sleep re-education”
approach can be summarized as follows.
Attitudes
- If you can’t sleep, don’t blame yourself . Putting pressure
on yourself only makes it that much harder to sleep.
- If you sleep
less than 8 hours, don’t assume that means you’re not getting enough
sleep. It’s counterproductive to expect to fall asleep when your head hits
the pillow and then sleep 8 hours straight every night.
-
Don’t let yourself get too upset about the situation.
- If you
get a bad night’s sleep, try to plan a pleasant activity when you start
your day. That way, you won’t get bogged down brooding about your sleep
habits, and you’ll prove to yourself that you can have a good day even if
you haven’t slept well.
Habits
-
Wait for the right time to go to bed; do so only when you feel very tired. If
you don’t fall asleep after 15 or 20 minutes, get up and get out of your
bedroom.
- Use your bed only for sleep or sex. Take the TV, reading materials,
and the telephone out of your bedroom. The idea is to create strong mental associations
between this room and sleeping.
- Make your biological clock more regular
by trying to get up at the same time every morning (even on weekends) regardless
of how many hours of sleep you got the night before.
- If you suffer
from insomnia, don’t take any naps during the daytime. Also, don’t
engage in any intense exercise, take a hot bath, or eat a heavy meal just before
going to bed, because all of these activities raise your body temperature, which
makes it harder to fall asleep. Do, however, take a lukewarm bath or shower, because
that relaxes your muscles, which can help you to sleep.
- Avoid tea,
coffee,
cola drinks, tobacco,
alcohol,
and other stimulants before going to bed.
- Eat an evening meal, neither
too light nor too heavy, and not too close to bedtime. Dairy products and some
herbal teas may also help you to sleep.
- Regular, moderate physical
exercise, not too close to bedtime, also helps you to sleep. It can be something
as simple as an evening walk through your neighbourhood.
- Instead of
worrying about whether you’ll be able to fall asleep, try to develop some
relaxing new habits associated with bedtime–reading or writing a bit, for
example–because they too can help you to sleep.
- Doing relaxation exercises
can help relieve tension that may be keeping you from falling asleep. Breathing
calmly and deeply, or listening to soothing music, will help you to relax. Anything
that calms you down and alleviates stress and anxiety
is conducive to sleep.
Compared with
sedatives,
this sleep re-education approach does a more effective job of modifying sleep
habits permanently. When people’s insomnia persists, taking sedatives for
a few days can help them get back into the habit of sleeping. But sedatives are
only a temporary solution, and a very imperfect one, because they can quickly
create a dependency, so that within a few weeks, they become an integral part
of the problem.
Most sedatives work by binding to GABA
receptors in the brain. In so doing, they inhibit the wakefulness network,
but they also disturb other circuits, such as those for mood and memory. Also,
sedatives often have side effects, such as tremors, or sleepiness during the daytime.
Thus the real solution is to re-learn how to sleep.
A 20-minute nap would
do most people good, because it would make them more alert and improve their ability
to concentrate. The psychological benefits in terms of their mood would also be
appreciable. But be careful: if you nap for too long (say, an hour), you will
go into too
deep a sleep, so you’ll feel sluggish for a while after you wake
up.
Naps are recommended for people who have accumulated a sleep deficit,
for people who are sleepy, and for people who suffer from certain sleep disorders,
such as narcolepsy.
But naps are not recommended for people with insomnia, because they can wind up
“borrowing” from their next night’s sleep.
Research
has shown that in extreme cases, such as when people have to drive alone and cannot
get several hours of sleep in a row, taking 10-to-20-minute naps at regular intervals
over the course of the day can partly meet their need for sleep and enable them
to perform at minimally acceptable levels for a few days. But their performance
under these conditions will always be far poorer than if they were completely
rested.
People who are performing monotous
tasks such as driving a vehicle for hundreds of kilometres may experience "micro-naps"
that last a few seconds. The frequency of these micro-naps is proportional to
the individual's sleep deficit, but they can also occur in people who have gotten
enough sleep, especially during cyclical
variations in alertness, such as those that occur about once
every 90 minutes.